Opening Hours
Mon 8am - 9pm
Tues 8am - 9pm
Wed 8am - 9pm
Thurs 8am - 9pm
Fri 8am - 9pm
Sat 8am - 5pm
Sun Closed
Search on Website
×
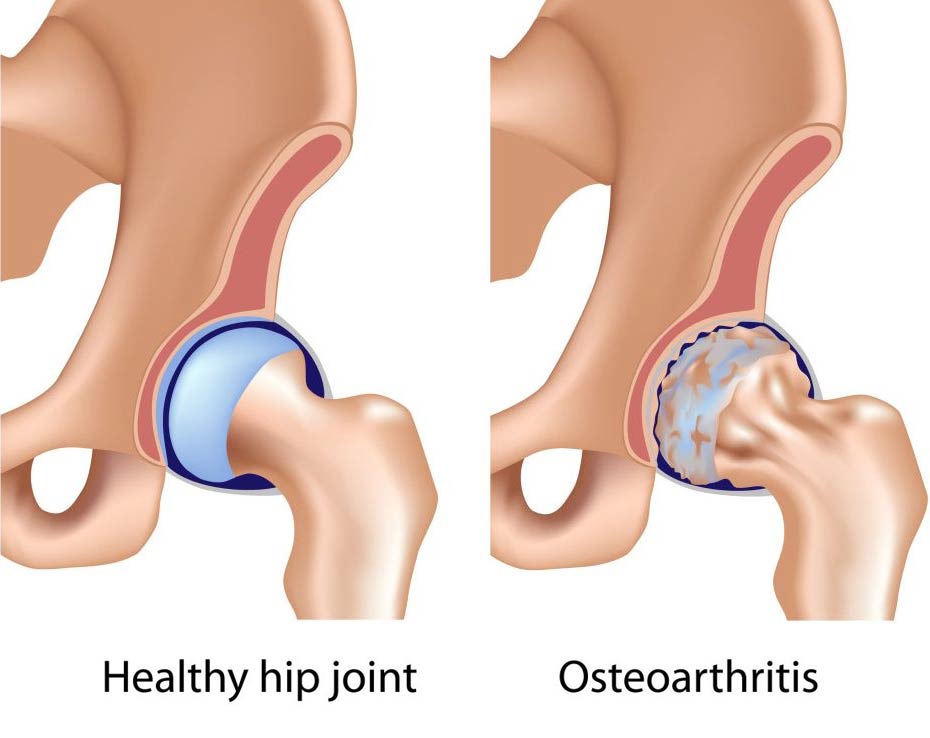
OA being the most common type, also known as wear and tear, causes damage to the cartilage that covers the bones in your joints. It affects around 85% of the population who are over forty five years of age. It can come on you gradually for no apparent reason or due to an old injury. OA is usually worse after activity and in the evenings and is relieved by rest.
RA occurs when your immune system mistakenly attacks the lining of your joints, causing a painful swelling that can eventually result in joint deformity. It affects females more than males most commonly around the thirty to forty age bracket. The onset can be sudden, you could actually wake up one morning and have RA, the reasons for this are not exactly known. However, 50% of cases have a genetic link, while having an abnormal reaction to bacteria or viruses are all possibly linked. A hormonal link is also considered because symptoms seem to improve during the third trimester of pregnancy and then two months post pregnancy can be more severe, but more research is needed in this area. Symptoms of RA leaves the person extremely fatigued and can come and go. Often sufferers complain of having a ‘flare up’.
OA’s diagnosis is based more on the person’s case history. They will typically complain of morning stiffness lasting less than thirty minutes and stiffness post inactivity. Swelling, reduced range of movement, joint deformity and muscle wasting are other signs associated. It affects the weight bearing joints for example, the hips, knees and lower back and is usually on one side. Cracking or crunching sounds are common signs and a sensation of giving way especially in the knees is a common complaint. Blood tests are not used to diagnose OA, but x-rays may reveal reduced joint space or deformity.
To diagnose RA, a person must experience at least four of the following six symptoms: morning stiffness for more than one hour, lasting more than six weeks; three or more joints affected, usually on both sides; swelling around joints for more than six weeks; changes with erosions especially in wrist hand and wrists, and an x-ray. Bloods are also taken to check for any inflammatory markers, which may lend more evidence to a diagnosis.
While both RA and OA can affect the small joints of the hand, there are differences. RA tends to affect the middle joints of the fingers and the joints where the fingers attach to the hand. The fingers will start to deform and drift out to the sides. OA more commonly affects the joints at the ends of the fingers and at the base of the thumb.
Manual therapy is very effective in decreasing pain and improving overall range of movement in suffers of OA. Good dietary advice and ways of improving your lifestyle will all help to slow down OA’s advances. Your doctor will advise use of non-steroidal anti-inflammatories, which are great at reducing pain, but long term use may cause stomach upset. Surgery is not recommended until one has a prolonged period of manual treatment.
To-date there is no known cure for RA. However, early diagnosis is important in prevention of damage to joints. How a person faces this terrible condition has a huge baring on its progression. Start by becoming highly educated around this condition and developing a long term ‘self-care’ plan, which should include a balance between rest and activity. Try to eat a healthy, balanced diet. It should be low in saturated fat, cholesterol, salt, and high in fibre and complex carbohydrate (whole grains, beans, fruits, and vegetables). According to some studies, fish oil may improve symptoms. Medication can be highly effective in slowing down the destruction of joints and reducing pain. People with RA have a higher risk of heart disease, and, therefore, anyone who smokes should stop immediately, as smoking increases this risk even more.
Stephen McDermott – Osteopath








